Healthcare revenue cycle · medical billing · 2026
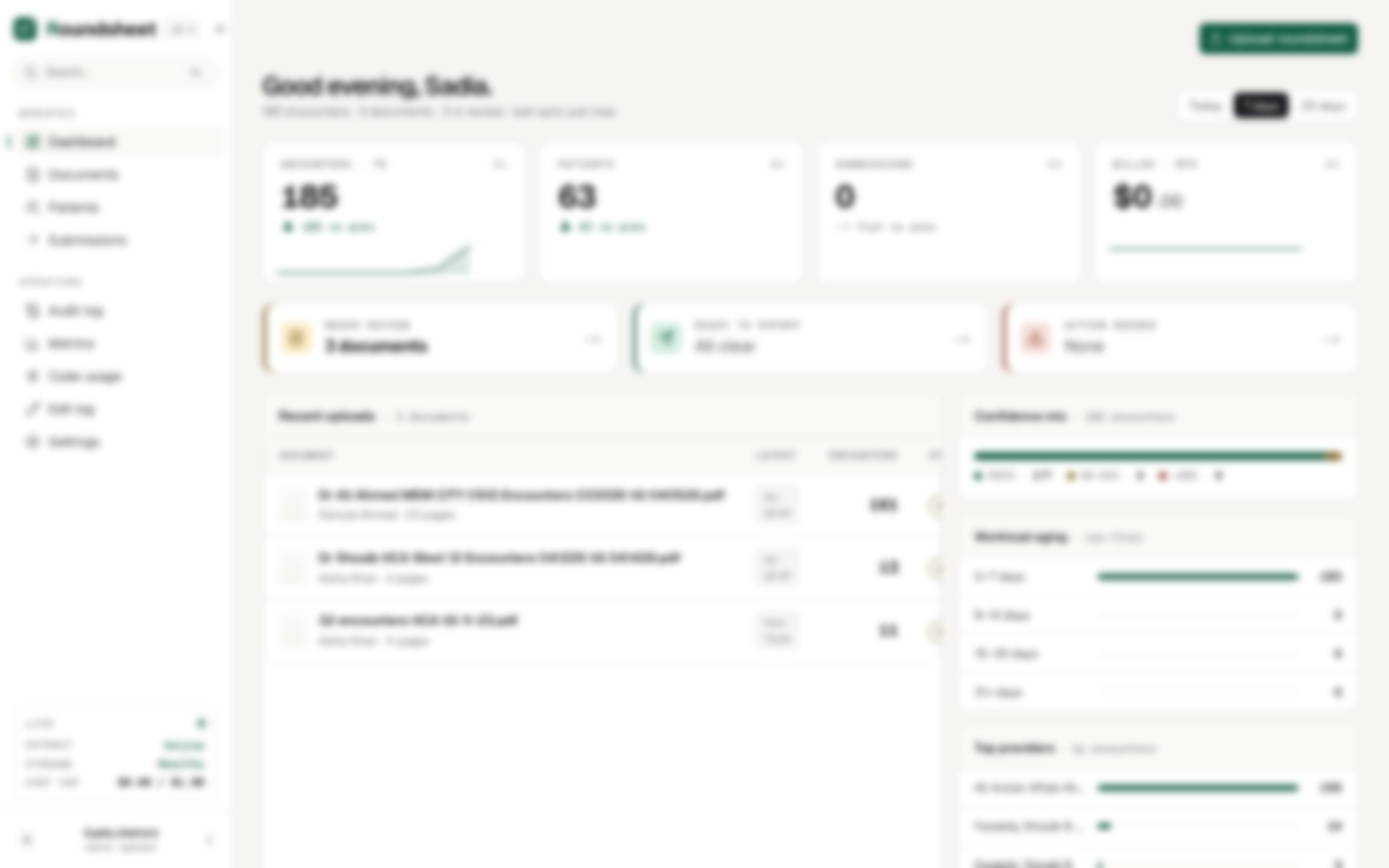
Billing platform that replaces the manual transcription bottleneck between hospital rounds and clearinghouse submission. Offshore billing reviewers upload marked-up census PDFs: handwritten attending notes, strike-throughs, room and bed scrawls, ICD-10 shorthand. Our vision models lift every encounter on the page into clean, structured data: patient, MRN, date of service, attending, diagnoses, codes, modifiers, units, place of service. Each field carries a confidence score and a box drawn back to the exact pixel it came from, sized to the page so the highlight lands on the right cell whether the scan is Letter, Legal, or A4.
The pipeline reads a page the way the billing floor does. It recognizes the common census layouts, settles who the billing attending is from the page as a whole rather than a single row, and sends clean typed pages down a cheaper path so the heavier model is saved for true handwriting, all under a fixed cost ceiling per document. Struck-through entries come through marked as rejected, visible to the reviewer and kept off the claim.
Eight checks run before anything is sent: code-versus-diagnosis sanity, retired codes, ICD-10 validity against the live CMS dictionary, fuzzy payer matching, continuity across multi-day stays, non-billable parent codes, CMS bundling and frequency edits, and a live provider-ID check. The last gate is a full round trip: the finished claim is re-read against the official 837P standard and held back if it will not pass. Approved encounters then merge into a real X12 837P file, one patient across several rounding days becoming a single claim with one line per day. When a payer responds, a closed loop reads the denial codes, sorts the disputes, and rebuilds the corrected claim without anyone leaving the tool.